
Quick Answer: When Blockchain Fits In Healthcare
Blockchain in healthcare fits when several independent organizations need a shared, tamper-evident record of events and no single party should own the whole history. The strongest use cases are patient consent proofs, provider credential attestations, drug and medical-device supply chain events, clinical trial audit trails, and cross-organization claims or authorization milestones.
It is not a default replacement for an EHR, claims platform, data warehouse, patient app database, or integration layer. Most healthcare software still needs governed databases, FHIR APIs, identity matching, access controls, encryption, audit logs, backups, and operational workflows. A ledger earns its place only when shared trust, provenance, and multi-party verification matter more than speed, simplicity, and editability.
The safest default is to keep protected health information off-chain. Store PHI in controlled clinical, document, or operational systems, then place only hashes, pointers, consent state, credential attestations, and timestamped workflow events on the ledger. That gives teams verification without turning sensitive records into permanent distributed data.
For teams evaluating a product build, NextPage's custom software development process should start with the trust problem, data sensitivity model, and integration map before a blockchain vendor is selected.
Why Healthcare Teams Consider Blockchain
Healthcare data moves across providers, payers, labs, pharmacies, device makers, patients, public health systems, and technology vendors. Each party has its own system of record, permissions, audit needs, and commercial incentives. That fragmentation is why blockchain attracts attention: it promises a shared history that participants can verify without manually reconciling every record.
The reference article from SparxIT presents broad healthcare blockchain benefits, use cases, trends, and business opportunities. This NextPage version takes a stricter engineering view: what problem is blockchain solving, who needs to verify the record, where does sensitive data live, and what simpler architecture would work just as well?
That distinction matters because healthcare is not a generic data-sharing environment. The HHS HIPAA Security Rule expects covered entities and business associates to protect electronic protected health information with administrative, physical, and technical safeguards. ONC's TEFCA work and CMS interoperability rules also show that national health data exchange is being shaped by governance, policy, APIs, and trust frameworks. A blockchain project has to fit that reality rather than route around it.
Practical Blockchain In Healthcare Use Cases
The strongest use cases involve records of events, permissions, provenance, or transactions that multiple parties need to verify. They are usually adjacent to clinical data, not replacements for clinical systems themselves.
| Use Case | Ledger Role | What Stays Off-Chain | First Success Metric |
|---|---|---|---|
| Patient consent and data-sharing preferences | Record consent state, revocations, timestamps, and policy versions | Medical records, identity documents, clinical notes | Fewer manual consent checks and cleaner audit history |
| Provider credentialing | Verify licenses, attestations, credential updates, and issuer history | Full HR files, background checks, private documents | Shorter credential verification cycle |
| Drug and device supply chain | Track custody events, batch proofs, recalls, and authenticity signals | Commercial contracts, private order details, patient records | Faster traceability during recalls or suspected counterfeit events |
| Clinical trial records | Timestamp protocol changes, consent events, data access, and result submissions | Participant PHI and raw clinical datasets | Stronger provenance and easier audit preparation |
| Claims coordination | Share status events, authorization milestones, and evidence hashes across parties | Full claim file, payment data, clinical attachments | Lower reconciliation effort between payer and provider systems |
These workflows all have a common thread: the ledger records evidence about a process. The operational data remains in systems built for privacy, search, reporting, edits, retention, and user experience.
Privacy And Compliance Risks
Healthcare blockchain projects fail when teams treat immutability as a universal good. In healthcare, records may need correction, retention controls, access restrictions, breach response, and jurisdiction-specific handling. A permanent distributed record can create risk if sensitive data, identifiers, or linkable metadata are written without a governance model.
HIPAA does not ban modern architectures, but it does require risk analysis and safeguards for electronic protected health information. The practical implication is simple: design the ledger as a proof and coordination layer, not as the place where clinical records live. Use encryption, key management, access controls, minimum necessary data flows, and strong off-chain storage policies.
Teams also need to think about metadata. A transaction that does not contain a diagnosis can still reveal that a patient interacted with a specialty clinic, payer, pharmacy, or medical device workflow. Privacy review should include direct data, indirect identifiers, participant visibility, node operators, logs, analytics, support access, and vendor roles.
If the project touches patient-facing workflows, use NextPage's healthcare software development company checklist to assess whether the delivery partner can reason through privacy, security, integrations, QA, and release controls before the blockchain layer is discussed.
Healthcare Blockchain Fit Matrix
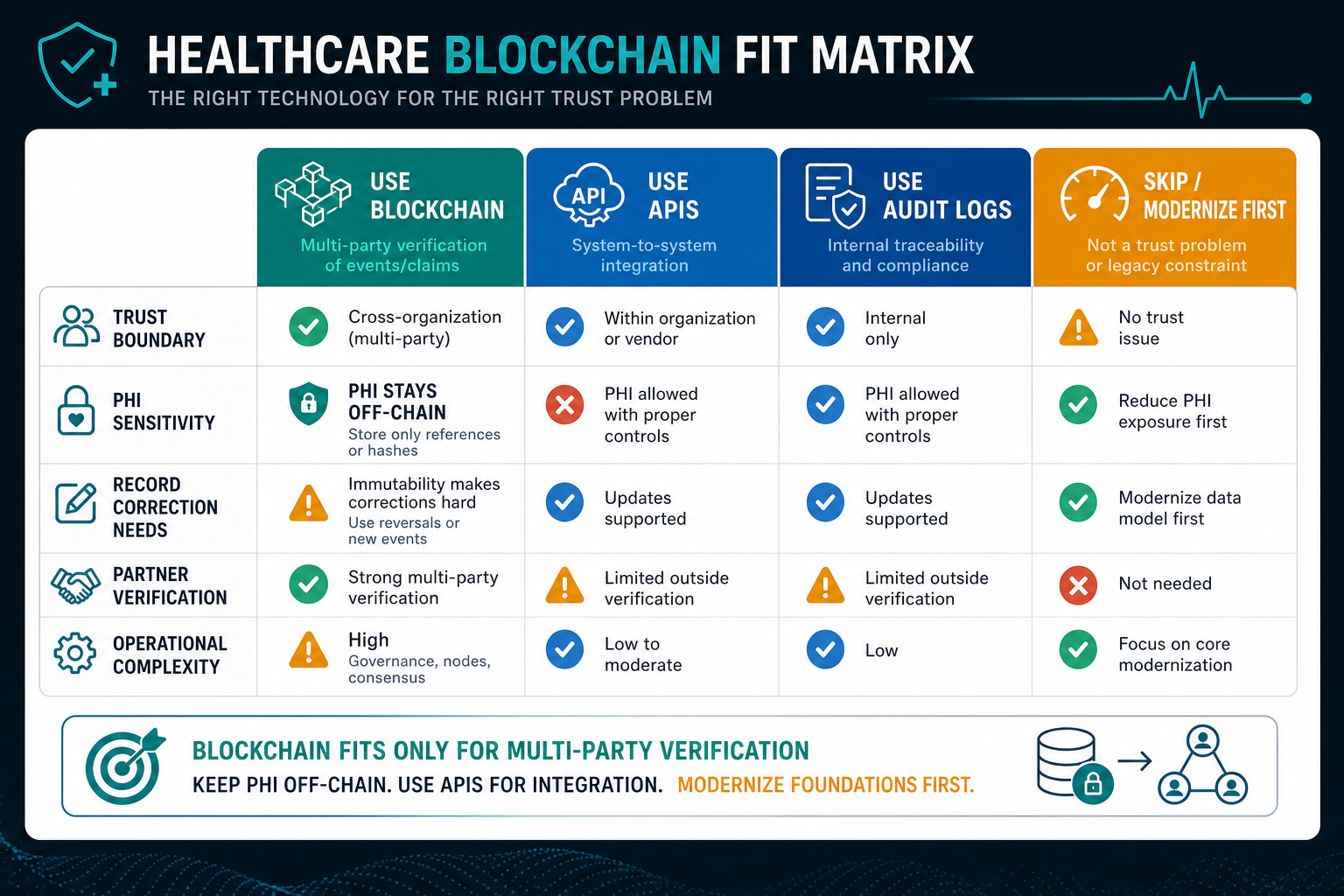
A useful fit test starts with four questions:
- Who must verify the record? If one organization owns the workflow, a database plus audit log is usually simpler.
- What data is being shared? If the workflow involves PHI, store sensitive data off-chain and keep only proofs or references on-chain.
- Can records change? If corrections, deletions, or retention rules are central, avoid irreversible sensitive entries.
- Is the problem really interoperability? If the main need is exchange between systems, modern APIs, event streams, or TEFCA-aligned exchange paths may be the better foundation.
For healthtech founders, this fit test should happen before vendor selection. A blockchain proof of concept may look impressive, but production value depends on identity, access control, integration, exception handling, audit reporting, and operational ownership.
The Build Vs Buy Decision Tool is useful when the question is whether to buy a mature network, integrate existing systems, modernize an old workflow, or build a custom proof layer.
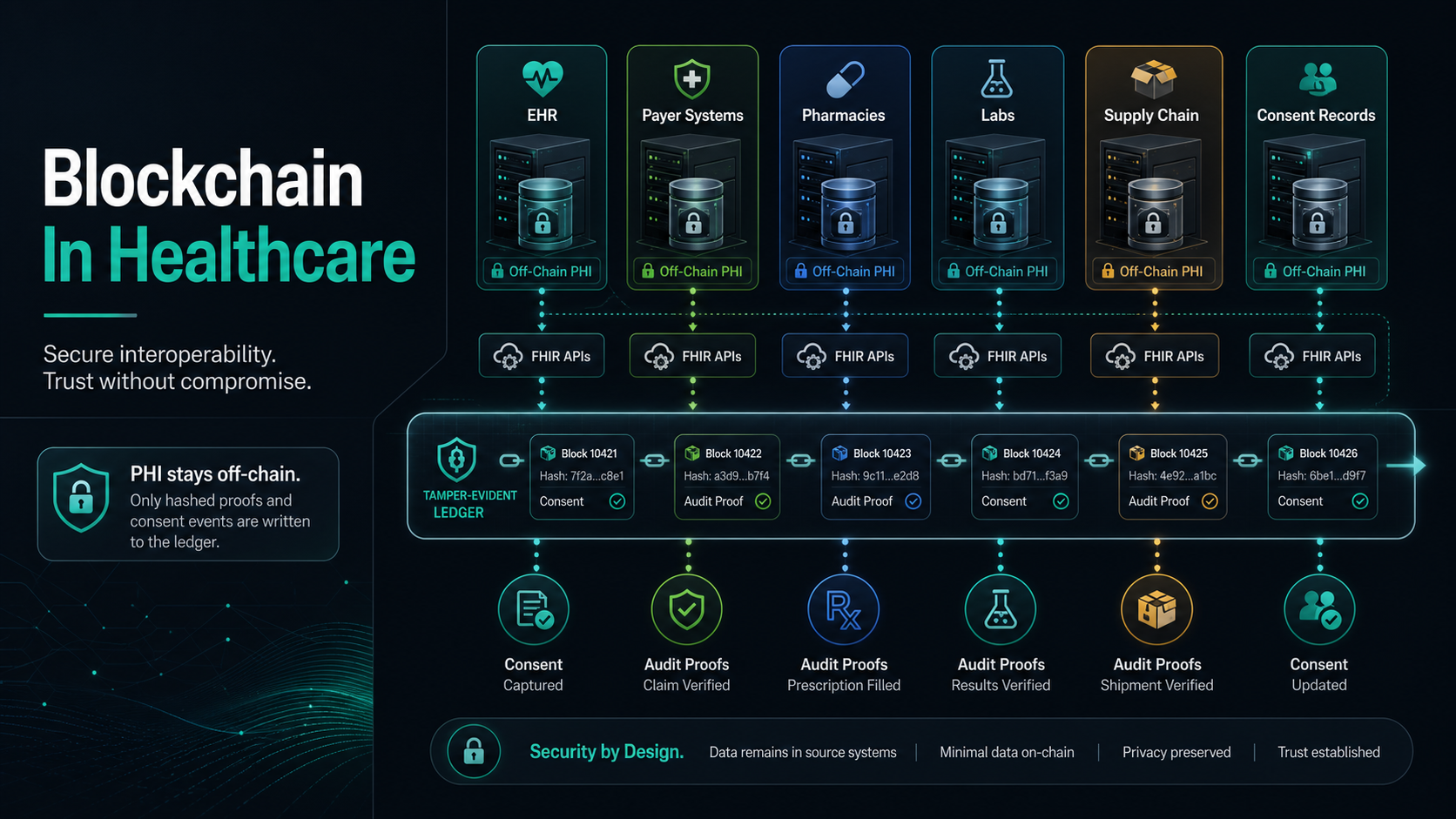
A Safer Healthcare Blockchain Architecture Pattern
A pragmatic architecture separates the healthcare workflow into four layers. First, clinical and operational systems hold PHI and business records. Second, an integration layer normalizes events from EHR, claims, CRM, lab, pharmacy, document, or device systems. Third, a governance layer handles identity, permissions, consent, key management, and policy decisions. Fourth, the ledger stores minimal verifiable events.
That architecture keeps the ledger narrow. For example, a consent workflow might store the consent version, timestamp, issuer, subject reference, hash of the signed artifact, and revocation state. The signed artifact itself stays in encrypted storage controlled by the healthcare organization. A credentialing workflow might store an issuer proof and status event while detailed credential files remain in a secure provider management system.
This is where custom software engineering matters. The ledger is rarely the hardest part. The difficult work is integrating existing systems, designing usable review screens, enforcing permissions, preparing audit exports, and making sure exceptions do not break the workflow.
For older healthcare platforms, the first move may be legacy software modernization: clean APIs, role-based permissions, audit trails, data cleanup, and secure hosting. Blockchain should not be used to hide brittle foundations.
Interoperability Reality: Blockchain Is Not A Shortcut
Many healthcare blockchain ideas are really interoperability ideas. A patient record exchange problem may need identity matching, consent, FHIR APIs, data normalization, governance agreements, and participation in trusted exchange networks. A ledger can complement those pieces, but it does not automatically solve semantic interoperability, patient matching, or data quality.
ONC describes TEFCA as a national approach that establishes a common governance, policy, and technical foundation for exchanging health information. CMS interoperability and prior authorization rules also push covered payers and partners toward API-based data exchange. For a healthcare operator, the architecture question is not "blockchain or no blockchain" in isolation. It is how the product will participate in real exchange workflows, respect patient access and privacy expectations, and avoid creating another disconnected data island.
If the product goal is better data movement between systems, start with integration design. Map the source systems, data formats, consent requirements, identity model, exchange partners, and failure modes. Then decide whether a ledger adds verifiable state that APIs and audit logs cannot provide.
The related NextPage guide to healthcare data exchange software development is the better starting point when the real problem is FHIR integration, partner onboarding, or operational data flow.
Medical Devices, IoT, And Supply Chain
Healthcare device ecosystems create another possible fit: device provenance, update history, maintenance events, software component attestations, and supply chain custody. The FDA's medical device cybersecurity materials emphasize that connected devices and hospital networks require lifecycle cybersecurity attention. That context makes provenance and update traceability valuable, but it also raises the bar for secure implementation.
A ledger can record that a device shipment changed custody, a firmware update was issued, a maintenance action occurred, or a batch was recalled. It should not become the control plane that delays urgent security patches or exposes operational details to participants that do not need them.
For IoT-heavy healthcare products, pair provenance with practical security engineering: device identity, secure update channels, SBOM handling where relevant, vulnerability response, monitoring, and incident workflows. Blockchain is at most one part of that control set. NextPage's IoT mobile app development roadmap is useful when device workflows, mobile surfaces, and cloud telemetry need to be planned together.
Build, Buy, Or Skip Blockchain?
Buy when a mature network already covers the workflow, has credible healthcare participants, offers strong governance, and integrates with your existing systems. Build when the trust model is unique, the workflow is a differentiator, or you need a custom operating layer around identity, consent, and auditability. Skip blockchain when one organization owns the workflow, participants do not need shared verification, records must be frequently edited, or the main bottleneck is integration rather than trust.
A common production pattern is hybrid. Use existing healthcare standards and APIs for data movement, conventional databases for operations, secure object storage for documents, and a narrow ledger for proof of consent, provenance, or multi-party status. This avoids using blockchain as a database while still capturing the benefit of verifiable shared state.
If the main uncertainty is whether a product should start as a proof of concept, pilot, or production MVP, the MVP Scope Builder can help turn the idea into a release boundary before engineering starts. For budget context around the surrounding product work, see the healthcare app development cost guide.
Pilot Scorecard Before Production Investment
A healthcare blockchain pilot should prove adoption and operational value, not only technical feasibility. A working ledger demo is not enough if partners will not onboard, support teams cannot resolve exceptions, privacy reviewers reject the data model, or the workflow takes longer than the old process.
| Pilot Question | Evidence To Collect | Decision Signal |
|---|---|---|
| Does the ledger solve a trust problem? | Named parties, disputed records, reconciliation pain, and verification needs | Continue only if multiple parties need independent verification |
| Is PHI controlled? | Data classification, off-chain storage, hashes, metadata review, retention model | Stop if sensitive data or linkable metadata lands on-chain without governance |
| Can partners operate it? | Onboarding steps, node or network responsibilities, support paths, exception workflows | Revise if partner burden is higher than the value created |
| Does it improve a metric? | Credentialing cycle time, consent audit effort, recall traceability, claims reconciliation | Scale only when measured value beats API or audit-log alternatives |
| Can it be secured and audited? | Key management, access controls, logs, vendor duties, incident response, test evidence | Do not scale without a clear operating owner |
For regulated or critical workflows, pair the pilot with governance controls. The NextPage post on AI governance for critical infrastructure software is not a blockchain article, but its risk-owner, audit-evidence, and control-mapping mindset applies to healthcare systems that cannot fail quietly.
Implementation Roadmap
Start with one workflow and one trust problem. For example: provider credential verification across clinics, consent proof for data sharing, or supply chain custody for a high-risk device category. Write down the parties, events, data sensitivity, dispute process, and owner of each decision.
- Define the trust boundary. Identify which parties must verify the history and why a single system owner is insufficient.
- Classify the data. Separate PHI, identifiers, commercial data, public events, hashes, and metadata.
- Choose the architecture. Decide between database plus audit log, APIs and event streams, consortium ledger, or hybrid model.
- Prototype the workflow. Test identity, consent, event writing, read permissions, exception handling, and audit export.
- Validate compliance and security. Review HIPAA responsibilities, vendor roles, key management, breach response, and operational controls.
- Test integrations and failure paths. Prove retry behavior, partner downtime handling, duplicate events, role changes, key rotation, and audit exports.
- Scale only after adoption proof. Measure reconciliation time, audit effort, partner onboarding, user trust, and support burden.
Healthcare teams also need product-grade UX around the ledger. Patient consent, provider reviews, claims evidence, and recall workflows need clear screens, notifications, permissions, and admin tools. For adjacent workflow patterns, see NextPage's guides to doctor appointment booking app development and mobile app integrations.
Common Mistakes To Avoid
- Putting PHI on-chain: immutable sensitive data creates correction, privacy, breach-response, and retention problems.
- Using blockchain for single-owner workflows: a conventional database with audit logging is usually simpler when one organization controls the process.
- Ignoring metadata leakage: transaction timing, participant names, and specialty workflows can reveal sensitive context even without diagnoses.
- Confusing interoperability with provenance: FHIR APIs, exchange governance, data normalization, and identity matching still matter.
- Skipping partner operations: a ledger that partners will not maintain, trust, or use creates another disconnected system.
- Underbuilding security controls: key management, access reviews, incident response, and vendor duties need the same rigor as the rest of the healthcare platform.
When the workflow includes AI, advanced analytics, or model-generated summaries, pair this article with the LLM application security checklist so model outputs do not become another ungoverned data path.
How NextPage Can Help
NextPage can help healthcare teams evaluate whether blockchain belongs in a product architecture, design the off-chain/on-chain boundary, build integration workflows, and create the audit, consent, and review interfaces that make the system usable. The goal is not to force a ledger into every workflow. The goal is to choose the simplest architecture that satisfies the trust requirement.
A practical first engagement can produce a fit assessment, workflow map, data sensitivity model, architecture decision record, and MVP scope. From there, the build can focus on the pieces that matter: interoperability, privacy, access control, user experience, evidence trails, and measurable operational value.
If your team is evaluating a healthcare blockchain project, start with the trust problem. If the answer is really integration, reporting, or workflow automation, solve that directly. If the answer is shared verification across independent parties, blockchain may be worth a narrow, governed pilot.