
Quick Answer: Telemedicine App Development Cost
Telemedicine app development cost usually depends on the care model before it depends on the number of screens. A focused virtual visit MVP with patient onboarding, appointment booking, provider availability, secure video, payments, notifications, basic admin controls, and launch analytics can often be planned around $45,000-$110,000. A stronger virtual clinic platform with patient, provider, coordinator, and admin roles, secure messaging, clinical notes, EHR or FHIR integration, consent capture, audit logs, insurance or payment workflows, and support operations often moves into the $110,000-$260,000 range. A multi-specialty telehealth platform with AI intake, remote patient monitoring, e-prescribing, claims workflows, enterprise security evidence, data warehouse reporting, and high-availability cloud operations can move beyond $260,000 and into $500,000+.
For 2026 planning, the budget should also account for policy volatility and reimbursement workflows. CMS guidance updated on February 26, 2026 says Medicare telehealth flexibilities run through December 31, 2027 for broad originating-site access, while HHS telehealth policy updates continue to emphasize eligible provider rules and behavioral health exceptions. Product teams should treat eligibility, billing evidence, consent, provider licensure, and clinical documentation as build assumptions to validate during discovery, not as copy added after launch.
For 2026 planning, the budget should also account for policy volatility and reimbursement workflows. CMS guidance updated on February 26, 2026 says Medicare telehealth flexibilities run through December 31, 2027 for broad originating-site access, while HHS telehealth policy updates continue to emphasize eligible provider rules and behavioral health exceptions. Product teams should treat eligibility, billing evidence, consent, provider licensure, and clinical documentation as build assumptions to validate during discovery, not as copy added after launch.
Those ranges are planning bands, not fixed quotes. A behavioral health consultation app, a second-opinion platform, a chronic-care remote monitoring product, and a provider-group virtual clinic can all be called telemedicine, but their cost drivers are different. The estimate changes when you decide who owns clinical review, how visits are documented, whether video is recorded, which systems receive health data, what audit evidence is required, and whether AI makes suggestions that a clinician must review.
If you need a directional range before discovery, start with the Custom Software Cost Estimator. Then validate the assumptions with a product and architecture workshop focused on care workflows, data boundaries, integrations, and release risk.
What You Are Really Building
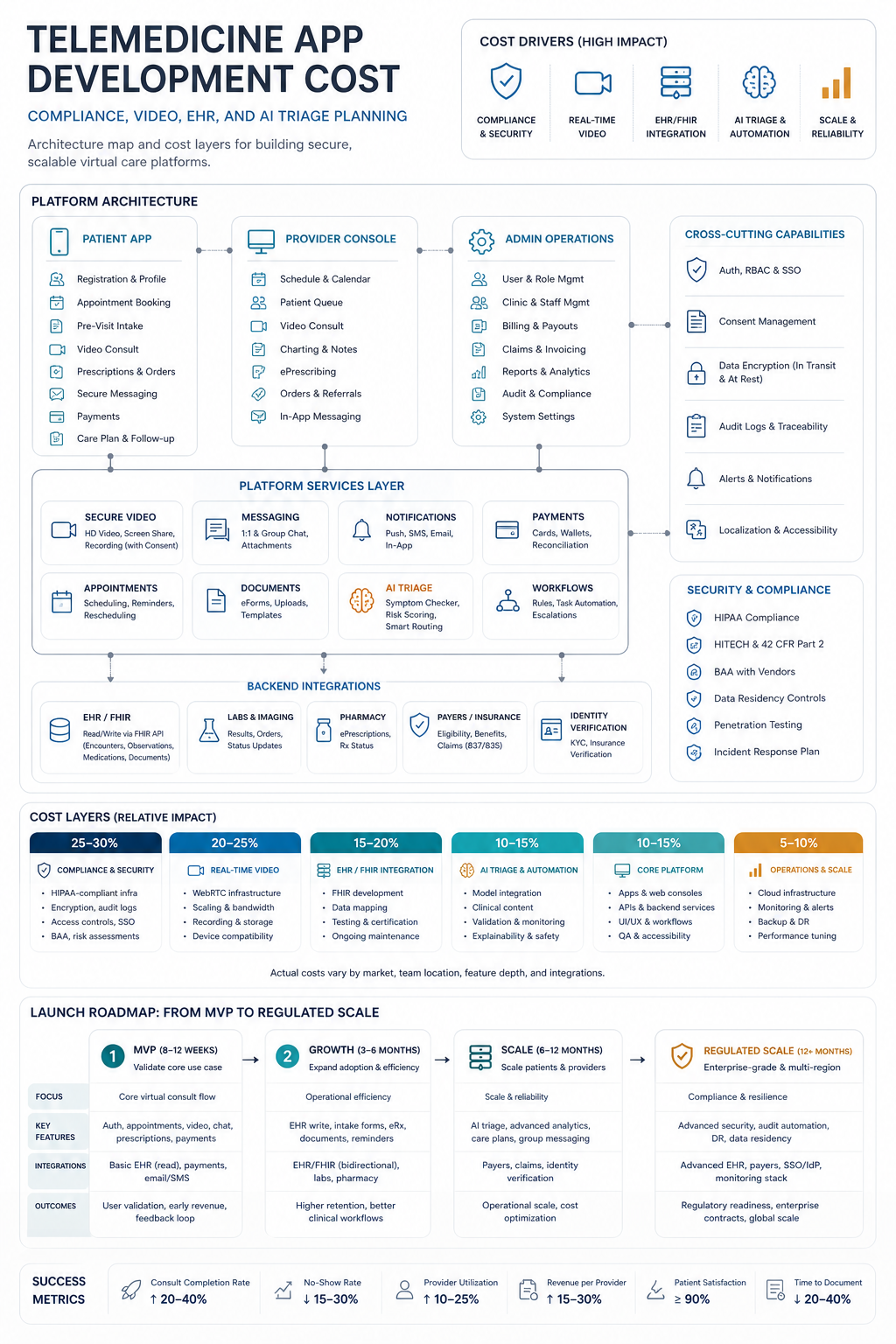
A telemedicine app is not just a video call with a login screen. It is usually a coordinated care workflow that connects patients, providers, operations teams, payments, records, notifications, support, security controls, and reporting. The visible patient app is only one part of the budget.
The first estimate question is what the product must safely enable. Store-and-forward telehealth may focus on intake forms, uploads, asynchronous review, and messaging. Scheduled video visits need availability, booking, pre-visit forms, waiting rooms, video session handling, notes, payments, and follow-up. A virtual clinic adds provider credentialing, care-team assignment, clinical documentation, support queues, admin reporting, and integrations. A remote monitoring or AI-assisted product adds data ingestion, thresholds, review queues, model evaluation, and escalation workflows.
This is why telemedicine is usually scoped as mobile app development, web app development, and secure provider/admin operating software. If the care workflow, data sensitivity, or integration depth is high, compare the scope with the broader Healthcare App Development Cost model before locking the first budget.
Cost Bands By Telemedicine Product Model
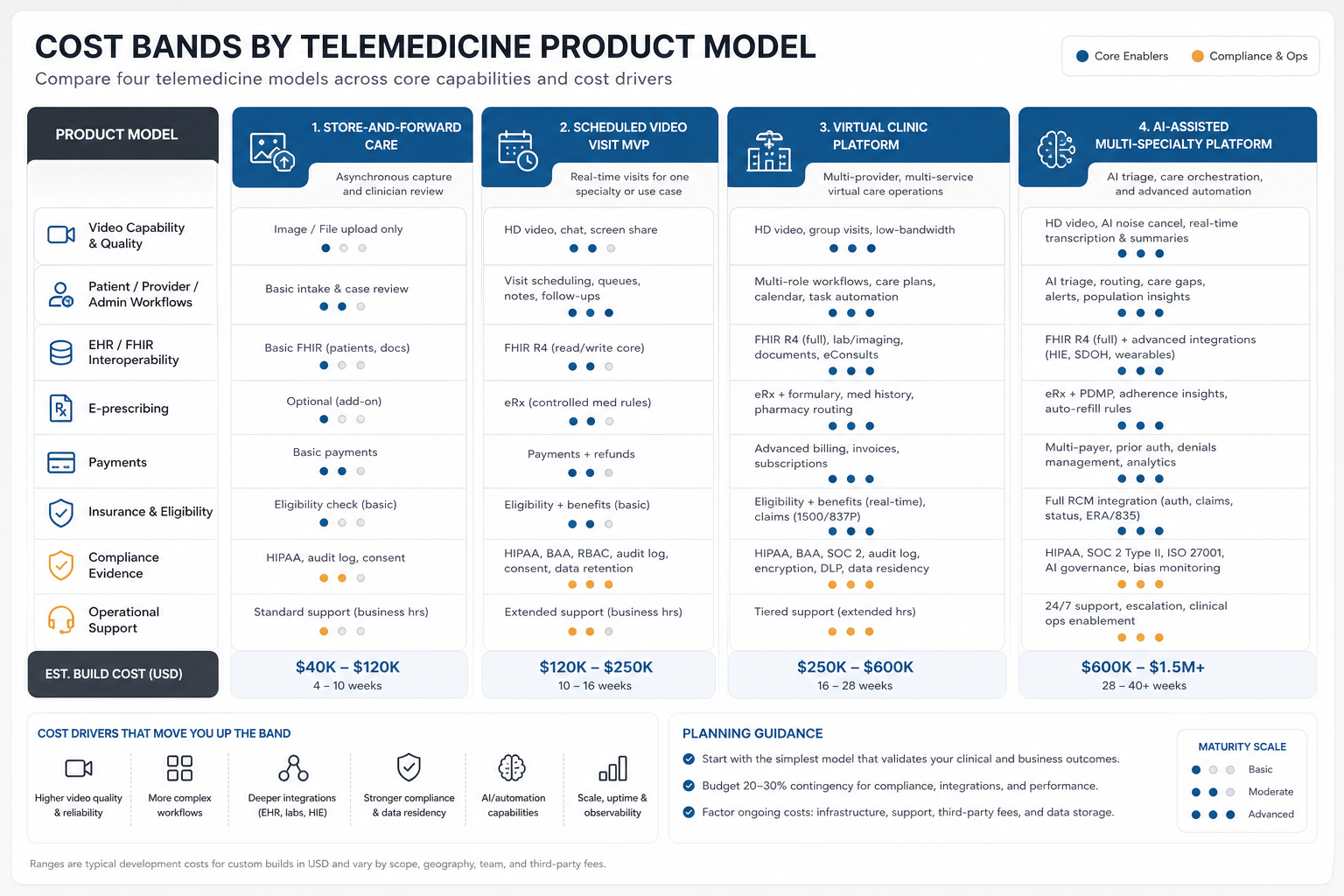
The clearest way to estimate telemedicine cost is to name the product model. A narrow MVP can be efficient when it proves one visit type for one audience. A platform becomes expensive when it needs multiple specialties, multiple care roles, deep EHR integration, claims, remote monitoring, or AI-supported intake.
| Product model | Typical first release | Planning range | What raises cost |
|---|---|---|---|
| Store-and-forward consultation | Patient intake, uploads, asynchronous provider review, secure messaging, payment, admin queue | $35,000-$85,000 | Complex forms, image/video uploads, specialty review rules, EHR writeback, clinical escalation |
| Scheduled video visit MVP | Patient app, provider availability, booking, payment, video visit, notes, reminders, basic admin | $45,000-$110,000 | Native apps, high-quality video, waiting room, consent, session events, provider portal depth |
| Virtual clinic platform | Patient, provider, coordinator, admin roles, secure chat, clinical notes, reporting, integrations | $110,000-$260,000 | EHR/FHIR, e-prescribing, payer workflows, support queues, role-based permissions, analytics |
| AI-assisted multi-specialty platform | AI intake, triage support, remote monitoring, specialty workflows, data warehouse, governance | $260,000-$500,000+ | Model evaluation, clinician review, device data, enterprise security, high availability, compliance evidence |
The SparxIT reference page positions telemedicine as a high-demand healthcare software category. NextPage's estimate model goes deeper into the operating choices that change budget: clinical workflow, data boundary, integration ownership, support tooling, and evidence requirements.
MVP Scope For Patient, Provider, And Admin Workflows
A useful telemedicine MVP should make one care journey reliable before it tries to serve every specialty. For patients, the MVP usually includes onboarding, profile, eligibility or location questions, appointment selection, intake forms, consent, reminders, payment, secure visit access, follow-up instructions, and support. For providers, it needs calendar controls, patient context, visit notes, messaging, simple disposition, and task handoff. For admins, it needs user management, provider availability, visit status, payment/refund handling, support visibility, and basic reporting.
The admin and provider sides often decide the real cost. A patient can join a visit with a simple interface, but the business still needs to manage no-shows, provider substitutions, rescheduling, clinical notes, payment exceptions, document uploads, support tickets, and operational reporting. A comparable lesson appears in Web App Development Cost: back-office roles and workflows can expand a project more than the public-facing screens.
Keep the first release narrow. Pick one visit type, one provider workflow, one payment or eligibility path, and one documentation model. Add specialties, care plans, RPM, claims, and deeper integrations after the first workflow proves demand and operational fit.
Secure Video And Messaging Decisions
Video is often treated as a single line item, but the decision has several layers: vendor selection, business associate agreement availability when applicable, waiting room behavior, participant identity, session tokens, device permissions, chat, screen sharing, recording policy, transcription, bandwidth handling, call-quality events, and support fallbacks. Buying video infrastructure through a proven provider is usually faster than building real-time communications from scratch, but integration and compliance work still need budget.
Telehealth.HHS.gov notes that covered providers and health plans must use telehealth technology vendors that comply with HIPAA Rules and will enter business associate agreements when required for video communication products or other remote technologies. HHS OCR guidance for remote communication technologies also highlights risk analysis questions around interception, encryption, recordings, transcripts, authentication, and session/device access. In engineering terms, that means the estimate should include vendor diligence, security configuration, logging, access control, and support playbooks, not only the video SDK.
Messaging adds similar decisions. Is it patient-provider chat, care-team chat, automated reminders, post-visit follow-up, or support messaging? Does it store PHI? Can patients attach files? Are messages part of the clinical record? Each answer changes retention, permissions, notification design, and integration requirements.
EHR, FHIR, And Third-Party Integrations
Integrations can be the largest hidden telemedicine cost driver. A low-scope MVP may start with payments, calendar, email, SMS, analytics, and a manual admin export. A virtual clinic may need EHR lookup, FHIR resources, document upload, e-prescribing, lab requests, identity verification, insurance eligibility, CRM, helpdesk, accounting, and data warehouse pipelines.
ONC describes FHIR as a widely used open standard for exchanging health information, and the Cures Act Final Rule calls for standardized APIs to help individuals securely access structured electronic health information with smartphone applications. Those standards can reduce friction, but they do not make integration free. Teams still need vendor access, authentication, scopes, data mapping, error handling, test patients, consent flows, monitoring, and support ownership.
A practical first-release rule is to integrate only where the workflow breaks without it. If the telemedicine product can safely launch with provider notes exported to an existing clinical system, delay bidirectional EHR writeback. If the product depends on medication lists, clinical history, or provider documentation inside the EHR, start FHIR and vendor discovery before finalizing the budget. Integration-heavy products often resemble Custom Software Development Cost projects because the expensive work lives in workflow reliability, not the app shell. When the roadmap includes custom clinical operations or enterprise workflows, compare the estimate with custom software development delivery assumptions before treating the mobile app as the whole product.
Compliance, Security, And Operational Evidence
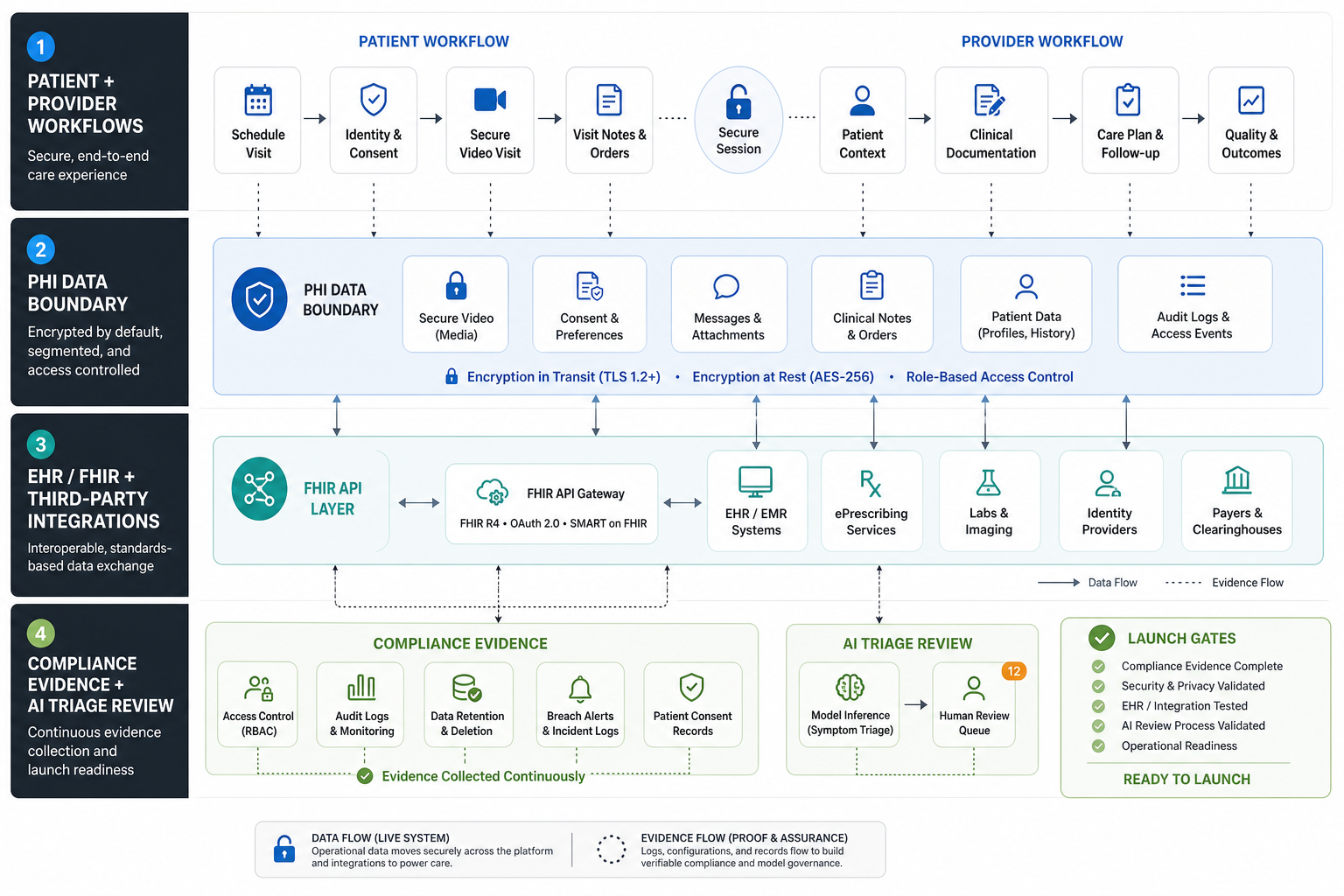
Telemedicine compliance is not a checkbox in the last sprint. It changes architecture, vendor choices, access controls, audit trails, environment separation, backup policy, incident response, retention, and internal operating procedures. HHS describes the HIPAA Security Rule as requiring administrative, physical, and technical safeguards for electronic protected health information. For telemedicine products, those safeguards often translate into role-based access, encryption, audit controls, session security, device and media rules, workforce access procedures, risk analysis, and vendor oversight.
This article is not legal advice. Exact obligations depend on geography, entity role, payer context, data flow, and whether the product is a covered entity, business associate, processor, or technology vendor. Engineering still needs to budget for the controls that the product, legal, compliance, and operations teams decide are required.
Operational evidence also matters. A buyer, clinic, enterprise customer, or auditor may ask how access is approved, how logs are reviewed, how incidents are handled, how backups are tested, how deployments are controlled, and how PHI is removed or retained. If those answers are important for sales or safe operations, they should be part of the estimate from day one.
AI Triage And Automation Scope
AI can make telemedicine workflows faster, but it can also add data, safety, and governance work. A simple AI assistant might classify intake reasons, summarize patient-provided symptoms for clinician review, draft follow-up instructions, or route support tickets. A higher-risk AI workflow might prioritize cases, suggest next steps, flag red symptoms, or support remote monitoring escalation. The second category needs stronger evaluation, review, monitoring, and escalation controls.
Use AI first where it reduces operational load without replacing clinical judgment. Intake summarization, missing-field prompts, provider note drafts, support routing, and post-visit education are often easier to govern than autonomous triage. If the AI feature saves coordinator time or improves routing, model the benefit with the AI Automation ROI Calculator and validate production controls against machine learning development services scope. If AI becomes part of the core care workflow, borrow architecture and governance patterns from AI Workflow Automation and healthcare-specific workflow patterns from Healthcare AI Agent Development.
Budget for retrieval sources, prompt/version management, red-team testing, evaluation sets, clinician feedback, human override, audit logs, and monitoring. AI is not just an API cost when the output influences patient experience or provider workload.
Timeline, Team, And Delivery Plan
A focused scheduled-video MVP usually takes 12-20 weeks after discovery when the team uses proven video, payment, notification, and cloud services. A virtual clinic platform often needs 20-36 weeks because patient, provider, coordinator, admin, support, and integration workflows must be tested together. AI-assisted, remote-monitoring, or multi-specialty platforms are usually delivered in phases over 6-12 months.
| Phase | Typical work | Output |
|---|---|---|
| Discovery and risk mapping | Care workflow, data boundary, user roles, compliance assumptions, integration targets, launch model | Estimate, architecture plan, MVP scope, release risks |
| UX and architecture | Patient journey, provider portal, admin workflows, video vendor, data model, security model | Prototype, technical plan, backlog |
| MVP build | Apps, backend, provider/admin tools, video, payments, messaging, analytics, deployment | Testable release candidate |
| Clinical and operational pilot | Visit testing, support scripts, security checks, provider feedback, workflow fixes | Pilot-ready product and go-live checklist |
| Growth releases | EHR/FHIR, automation, AI intake, reporting, RPM, hardening, enterprise evidence | Scalable platform roadmap |
The team usually includes a product lead, UX/UI designer, mobile or full-stack engineers, backend engineer, QA, DevOps/cloud support, and security/compliance-aware architecture support. Integration-heavy products also need vendor coordination and test data planning.
Budget Mistakes To Avoid
- Pricing only the patient app: provider portals, admin queues, support tools, audit logs, and reporting can be as important as the patient experience.
- Treating video as plug-and-play: session tokens, waiting rooms, identity, recording policy, vendor agreements, call quality, and fallbacks still require design and testing.
- Starting EHR integration too late: vendor access, FHIR scopes, data mapping, test patients, and error handling can change both timeline and budget.
- Overbuilding AI triage: start with assistive workflows and human review before funding high-risk automation.
- Ignoring operations: no-shows, refunds, provider substitution, support tickets, notes, and follow-up workflows need owners and tools.
- Leaving compliance evidence for the end: security controls, auditability, vendor review, and incident response are cheaper when designed early.
How NextPage Scopes Telemedicine Products
NextPage scopes telemedicine products by mapping the care journey before estimating screens. We define the patient workflow, provider workflow, admin responsibilities, data boundary, video and messaging approach, integration map, AI opportunities, compliance assumptions, and launch metrics. Then we split the roadmap into an MVP, a clinical pilot, and growth releases.
That may mean a lean scheduled-video MVP for one specialty, a virtual clinic platform for a provider group, an asynchronous second-opinion workflow, or an AI-assisted intake layer connected to existing systems. The goal is to put the first budget behind the workflow that proves demand and operational safety.
If you are planning a telemedicine product, use the Custom Software Cost Estimator for a first directional range. Then bring the care model, user roles, target geography, video requirements, EHR assumptions, AI ideas, and compliance constraints into a focused discovery sprint.