
Generative AI clinical documentation works best when it is designed as a reviewed clinical workflow, not as a free-form chatbot attached to patient records. The safest pattern is to capture the encounter context, keep protected health information inside governed boundaries, generate a draft note, route that draft to a clinician for review, and write only approved content back to the EHR.
That distinction matters. A clinical documentation assistant may reduce charting burden, improve note consistency, and help teams find missing context, but it also touches regulated data, clinical accountability, and integrations that cannot be handled with prompt design alone. Teams evaluating generative AI development for healthcare should scope the workflow, data controls, review loop, and EHR handoff before they compare models.
In 2026, the planning bar is higher than a basic AI-scribe proof of concept. ONC's HTI-1 materials put new attention on transparency for AI and predictive decision support inside certified health IT, HHS/OCR continues to frame AI through privacy, security, and nondiscrimination obligations, and health AI assurance groups such as CHAI emphasize evaluation, monitoring, and lifecycle governance. A clinical documentation assistant should therefore be scoped as regulated workflow software with evidence, not as an isolated prompt.
Quick Answer: Generative AI Clinical Documentation
A HIPAA-conscious generative AI clinical documentation workflow typically includes secure intake, role-aware PHI access, minimum necessary context, retrieval controls, draft generation, clinician review, EHR/FHIR mapping, audit logs, and ongoing quality monitoring. The AI should support documentation, summarization, coding preparation, handoff notes, and patient instructions only within approved workflows and with human signoff for medical-record updates.
For a first release, the strongest scope is usually narrow: one care setting, one note type, one EHR integration path, one review queue, and a small set of measurable outcomes. Trying to automate every specialty, every template, and every downstream task in the first version makes compliance review and clinical adoption harder.
What The Workflow Should Do
Start with the documentation job, not the model. A primary-care clinic may need SOAP-note drafting from transcript snippets and structured intake data. A specialist group may need prior-record summarization before the visit. A hospital team may need discharge summary preparation, handoff notes, or problem-list reconciliation. A healthtech product may need chart review support inside an existing clinical operations platform.
Those use cases share a common workflow: gather authorized context, normalize it, generate a draft, expose the sources used, collect clinician edits, write approved content to the system of record, and keep evidence of what happened. This is closer to AI workflow automation than to a standalone content-generation feature.
| Workflow Step | Product Decision | Control To Add |
|---|---|---|
| Capture | Transcript, typed notes, forms, labs, medication list, prior notes, or uploaded documents | Consent handling, data classification, and source provenance |
| Prepare context | Which fields and documents the model can see | Minimum necessary context, tenant filters, role filters, and redaction where appropriate |
| Generate draft | Note type, tone, template, structured sections, and citations | Prompt versioning, model versioning, and output schema validation |
| Review | Who approves, edits, rejects, or escalates | Clinician signoff, change tracking, confidence flags, and exception queues |
| Record | How approved content enters the EHR or downstream tool | FHIR/API mapping, audit event, retry logic, and rollback path |
HIPAA And PHI Controls To Design Before Model Selection
HIPAA does not make a model compliant by itself. HHS describes the HIPAA Security Rule as requiring appropriate administrative, physical, and technical safeguards for electronic protected health information. In product terms, that means the AI workflow needs access policy, security risk analysis, encryption decisions, identity controls, vendor review, logging, incident handling, and workforce procedures around the software.
Before choosing a model provider, decide where PHI is allowed to travel. Will the system use a HIPAA-eligible cloud service with a business associate agreement? Will inference run in a private environment? Can the model provider use prompts or outputs for training? How long are prompts, transcripts, embeddings, drafts, and logs retained? Which data enters analytics? Which fields are excluded from prompts?
Build the control map before model selection. The architecture should separate raw encounter data, approved clinical context, prompts, embeddings, draft notes, clinician edits, and audit evidence. Teams should also decide which components belong in the covered environment, which vendor contracts require business-associate terms, and where de-identification, retention, access review, and incident-response evidence will live.
Healthcare teams should also avoid placing secrets, broad policy text, or raw PHI into prompts as a shortcut. Prompt instructions are not an access-control layer. The surrounding application should enforce role access, tenant boundaries, source allowlists, output validation, and auditability. NextPage's LLM application security checklist is a useful adjacent control map for prompt injection, RAG risk, tool permissions, and logging.
For 2026 planning, treat HIPAA security analysis, vendor processing rules, and model telemetry as part of the product scope. If prompts, transcripts, embeddings, draft notes, or evaluation traces are retained, the team needs a reason, a retention window, and an access path for audit and deletion. If a vendor or model endpoint can use inputs for improvement outside the covered workflow, that is a contract and architecture decision, not a prompt-engineering detail.
If the product touches patient intake, triage, telehealth, or care-team handoff, review adjacent healthcare workflow constraints as well. NextPage's telemedicine app development cost guide is useful context for video, EHR, compliance, and AI-triage scope that often overlaps with documentation assistants.
EHR And FHIR Integration Decisions
FHIR helps teams exchange healthcare data through standardized resources, but FHIR alone does not define the entire clinical documentation product. HL7 describes FHIR as a specification built around resources that can be combined for use cases, and the web/API model makes it useful for modern EHR integrations. The implementation work is still in mapping, permissions, testing, error handling, and EHR-specific behavior.
For teams that need a production build rather than a prototype, this is where custom software development matters: the application layer has to own workflow state, identity, source provenance, review queues, retry handling, and integration behavior around the model.
For clinical documentation, common resources and concepts may include Patient, Practitioner, Encounter, Condition, MedicationRequest, Observation, DiagnosticReport, DocumentReference, Composition, and provenance or audit events depending on the system. Some EHRs expose robust APIs, some require partner approval, and some workflows still depend on HL7 v2 feeds, interface engines, or manual review exports.
HealthIT.gov's certification and information-blocking materials also matter because patient access and health information exchange expectations influence how software teams design APIs and data access. A practical implementation should document which API surfaces are available, which data can be read, which data can be written, and what approval is required before AI-assisted notes are committed.
Clinical-note implementation also needs a writeback policy. Some workflows should create a draft for copy-and-review only. Others can create a structured note, composition, document reference, task, or message that remains pending until the clinician signs it. The safer MVP records provenance for source snippets, generated text, clinician edits, model and prompt versions, and the final EHR write event so later review can explain how the note reached the chart.
Clinical AI Pilot Risk Register
Before a pilot reaches live patient workflows, document the failure modes the team will monitor and who is allowed to pause rollout. A clinical documentation assistant can look accurate while still omitting key context, copying irrelevant history, overstating certainty, or producing notes that are technically formatted but clinically incomplete. A simple risk register keeps the pilot grounded in reviewable evidence instead of model enthusiasm.
| Risk | Early Signal | Mitigation |
|---|---|---|
| Unsupported clinical statement | Draft includes a fact that is not present in the encounter, chart, or approved retrieval source | Show source references, require clinician signoff, and track unsupported-claim rate by note type |
| PHI overexposure | Prompts, logs, analytics, or support tools receive more patient context than the workflow needs | Enforce minimum necessary context, role filters, retention limits, and vendor-processing rules |
| EHR writeback mismatch | Approved notes fail mapping, duplicate fields, or land in the wrong section of the record | Start draft-only, test FHIR/API mappings, keep retry queues, and audit every writeback event |
| Adoption drift | Clinicians bypass review guidance or stop trusting the assistant after repeated rework | Measure edit distance, rejected drafts, satisfaction, and support tickets during each release window |
This risk register also clarifies when a workflow should remain a supervised copilot instead of becoming an agentic workflow. If the product roadmap includes autonomous task execution, pair this article with the AI Agent Readiness Assessment and the Generative AI vs AI Agents vs Agentic AI guide before giving the system tool access or write permissions.
Document the assurance evidence before expanding the pilot: intended use, excluded use, training or configuration data, evaluation set, subgroup performance checks where relevant, clinician override path, monitoring owner, and pause criteria. That evidence makes governance review concrete and helps the team decide whether the assistant is ready for more note types, more specialties, or deeper EHR permissions.
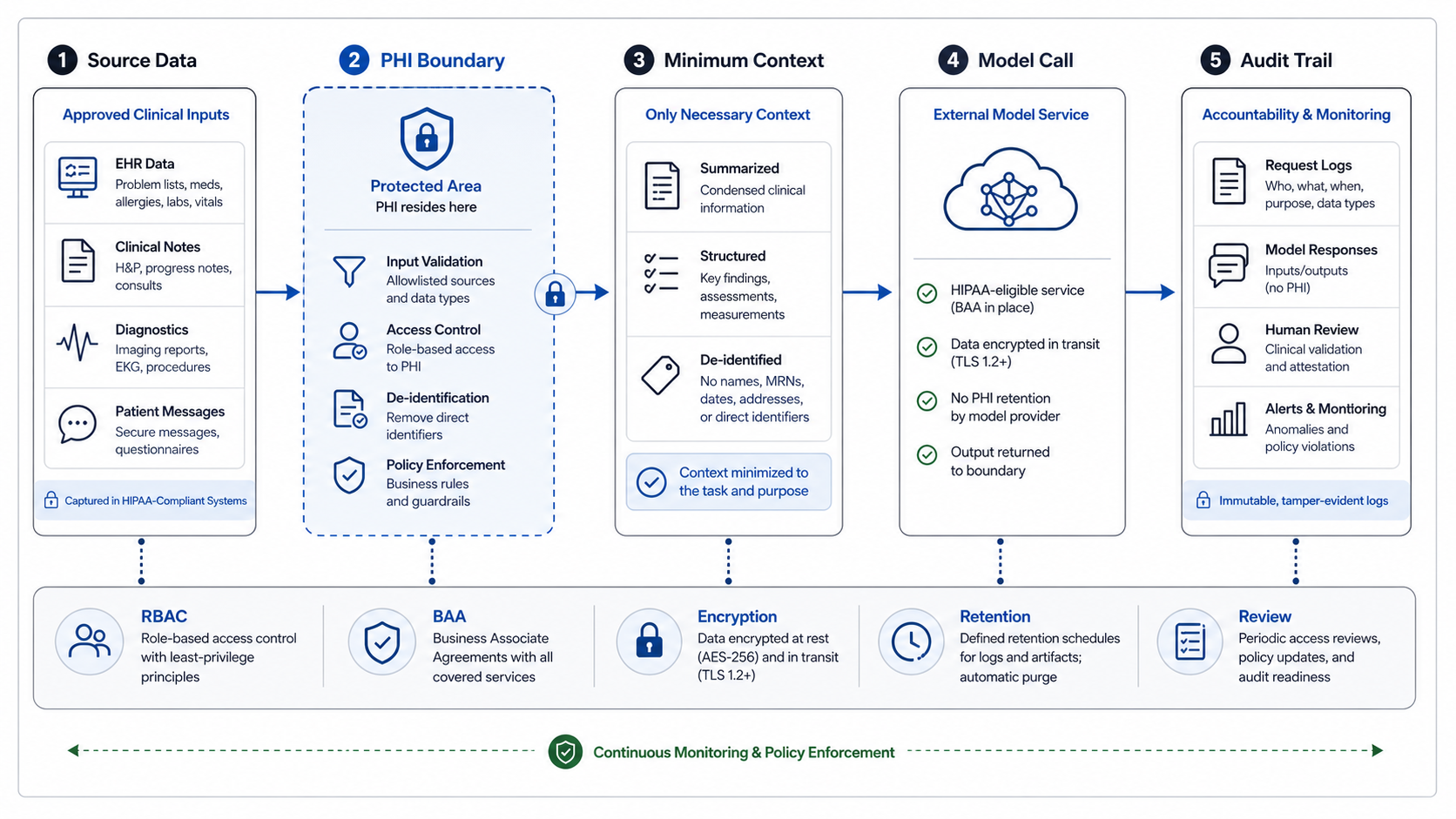
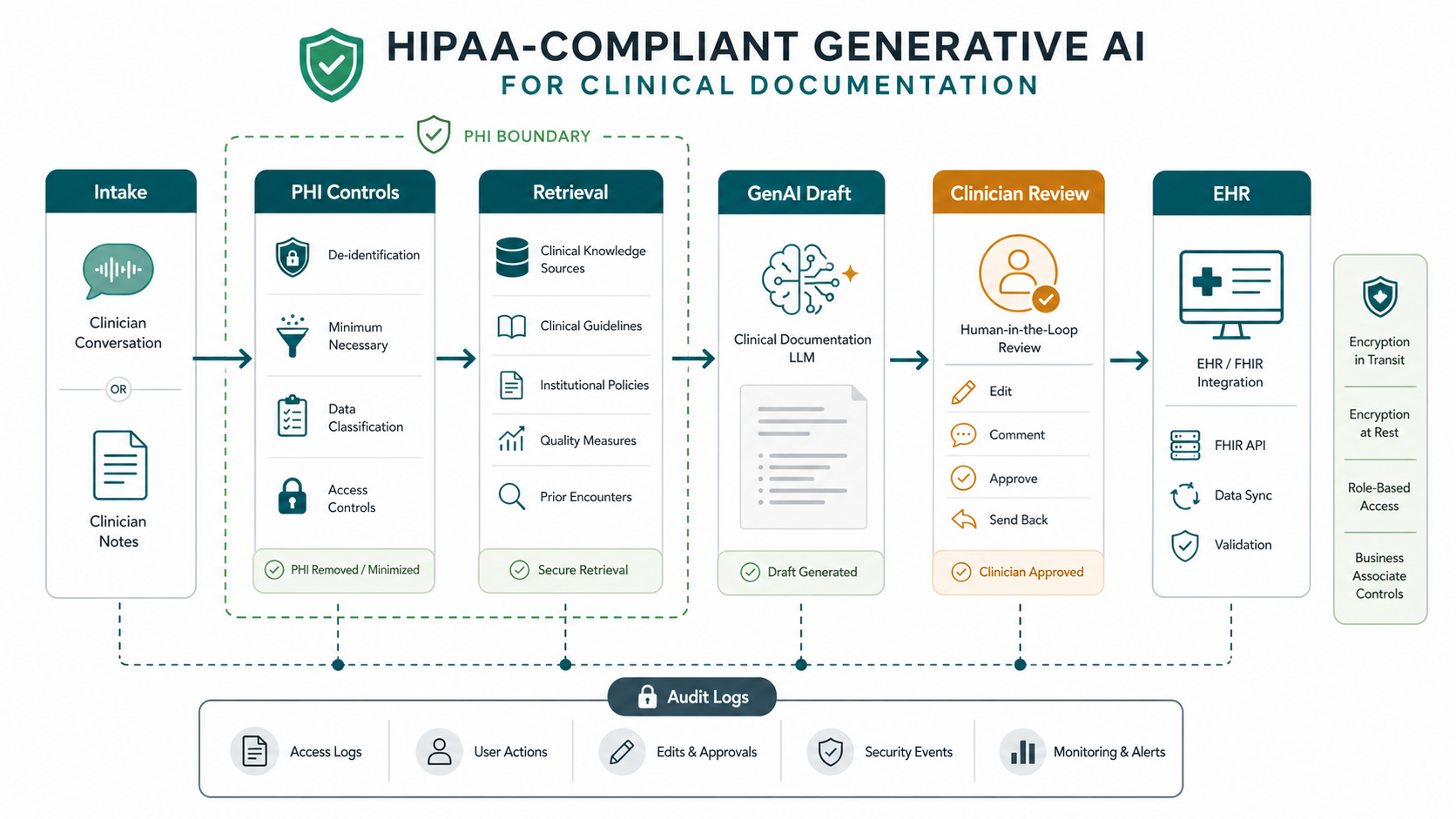
A Practical Architecture Pattern
The architecture should separate intake, data control, model orchestration, review, and system-of-record integration. Intake captures encounter context from approved sources. A control layer classifies data, checks authorization, limits context, and records provenance. A retrieval layer adds only relevant clinical context. The model produces a structured draft, not a final record. The clinician review surface highlights assumptions, missing data, uncertain language, and source references. The integration layer writes approved updates through the EHR's supported API or interface path.
This pattern also makes the buying conversation clearer. A team does not need to ask whether it needs "a healthcare AI app" in the abstract. It can ask which systems the assistant must read, which note templates it must support, how the review queue works, how PHI is handled, how output quality is measured, and what the first production workflow should include. That is the same scoping discipline used in strong healthcare software development company evaluations.
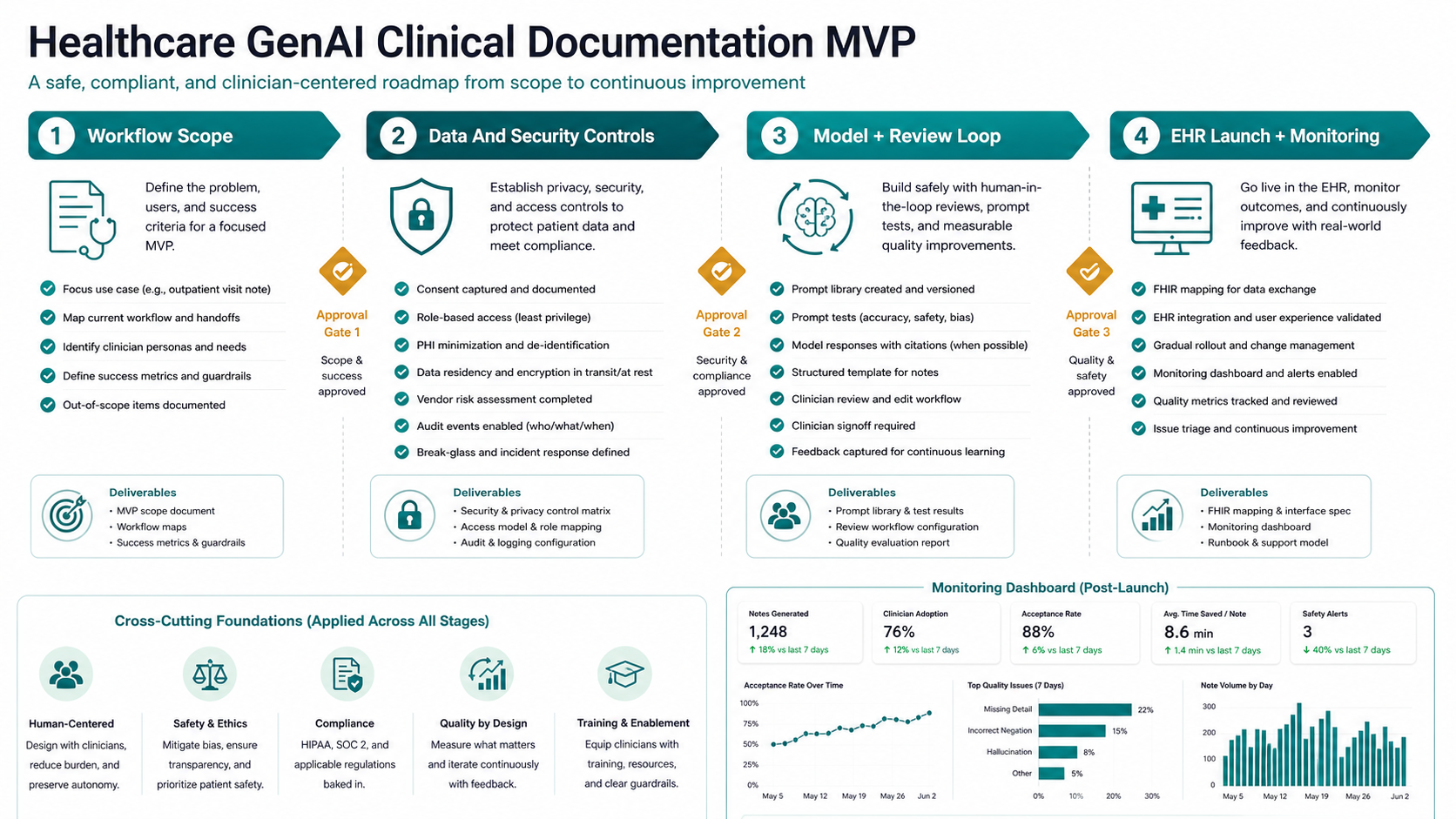
MVP Roadmap For A Clinical Documentation Assistant
Stage 1: workflow scope. Pick one documentation workflow, one user group, and one output format. Define the current pain: late charting, inconsistent notes, missing prior context, duplicated handoff work, or manual summarization. Identify the clinical owner who decides whether the output is good enough.
Stage 2: data and security controls. Map all PHI touchpoints: transcript capture, uploaded documents, EHR reads, retrieval index, prompts, model outputs, temporary files, audit logs, analytics, and support tooling. Decide retention, encryption, access, vendor, and deletion rules. If the broader product budget is still unclear, the healthcare app development cost guide can help frame compliance and integration cost drivers.
Stage 3: model and review loop. Build prompts, retrieval, templates, and validators around the selected note type. Track clinician edits as feedback, but avoid silently treating every edit as training data. Add test sets for omissions, hallucinated facts, wrong medication context, copied irrelevant history, and unsafe certainty.
Stage 4: EHR launch and monitoring. Start with a draft-and-review workflow before writeback automation. Add EHR writeback only after the team has stable mappings, user acceptance, audit events, retry handling, and rollback procedures. Measure note turnaround time, edit distance, clinician satisfaction, safety flags, rejected drafts, and support incidents.
Governance And Quality Metrics
Clinical documentation AI needs governance from the first pilot. Decide who owns model changes, prompt changes, template updates, retrieval source changes, and incident response. Keep release notes for the AI workflow just as you would for any regulated software feature. When outputs affect patient records, the review policy should be explicit: the clinician approves the final note, the AI does not practice medicine, and unresolved uncertainty is escalated instead of hidden.
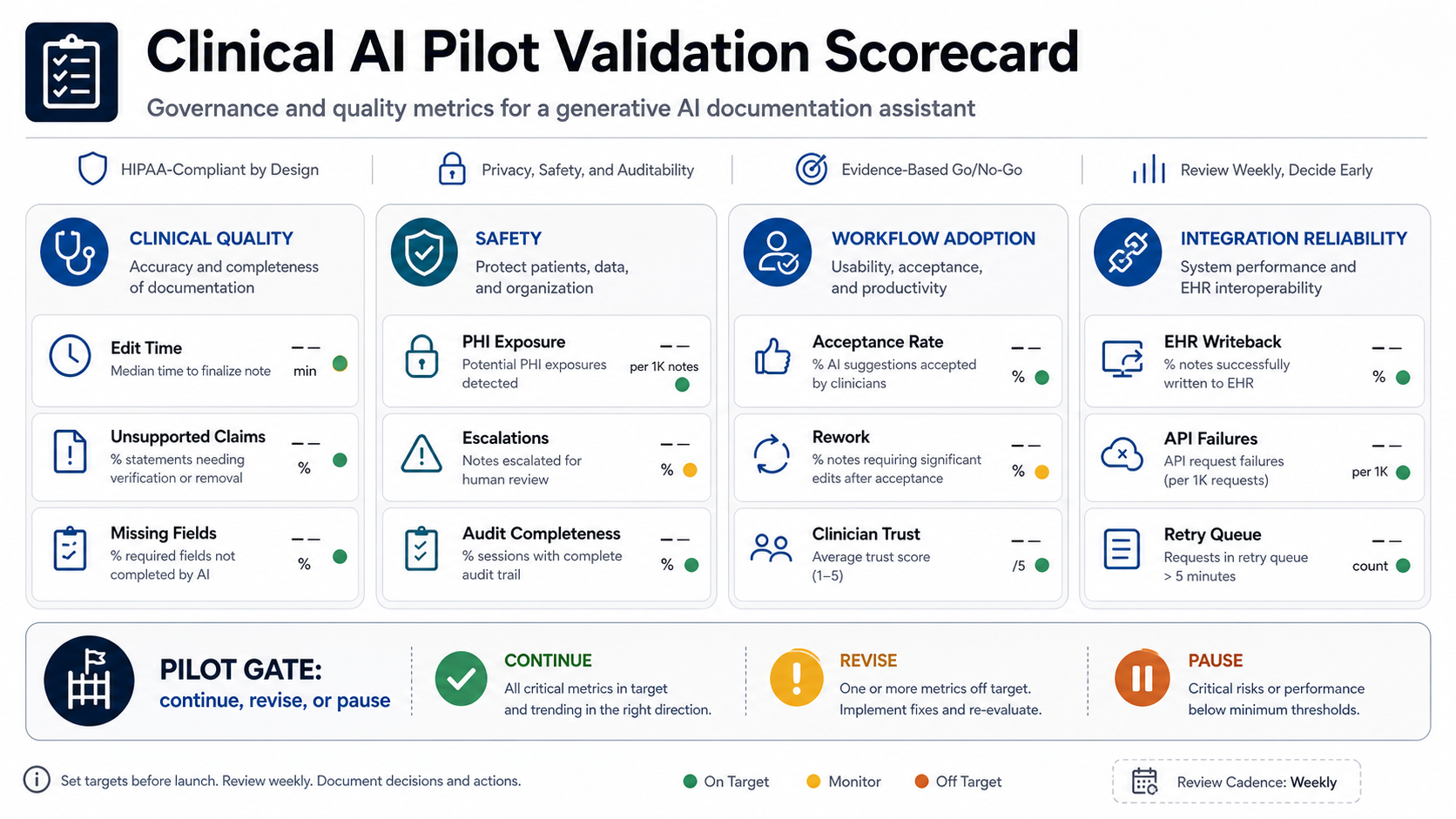
Useful quality metrics include draft acceptance rate, average clinician edit time, unsupported-claim rate, missing-key-field rate, complaint rate, note completion time, after-hours charting reduction, and EHR writeback failures. Useful security metrics include access-denied events, unusual prompt activity, retrieval misses, PHI redaction failures, audit-log completeness, and vendor processing exceptions.
Set release gates before launch. A pilot should pause when unsupported clinical statements cross the agreed threshold, when PHI appears in unapproved logs, when EHR writeback failures cannot be reconciled, or when clinicians reject drafts often enough that the assistant creates more work than it removes. It should expand only when quality, safety, adoption, and integration reliability are all moving in the right direction.
For operational planning, pair the clinical metrics with a benefits model. The AI Automation ROI Calculator can help estimate whether the targeted documentation workload is large enough to justify a pilot, while AI development services can help shape the secure workflow, integrations, and evaluation layer.
When To Build With NextPage
Build a custom clinical documentation assistant when your workflow is too specialized for generic AI scribe tools, your product needs EHR or internal-system integration, your data governance requirements are strict, or your roadmap includes a broader healthcare AI platform. Off-the-shelf tools can be useful, but they may not fit custom intake, specialty templates, approval logic, analytics, or multi-system workflows.
NextPage can help plan the architecture, build the secure application layer, connect EHR and internal systems, design review queues, and implement model evaluation. If your team is already considering LLM development or a broader clinical GenAI product, start with a healthcare AI readiness assessment: define the workflow, map PHI boundaries, validate integration access, and scope a pilot that clinicians can safely test.