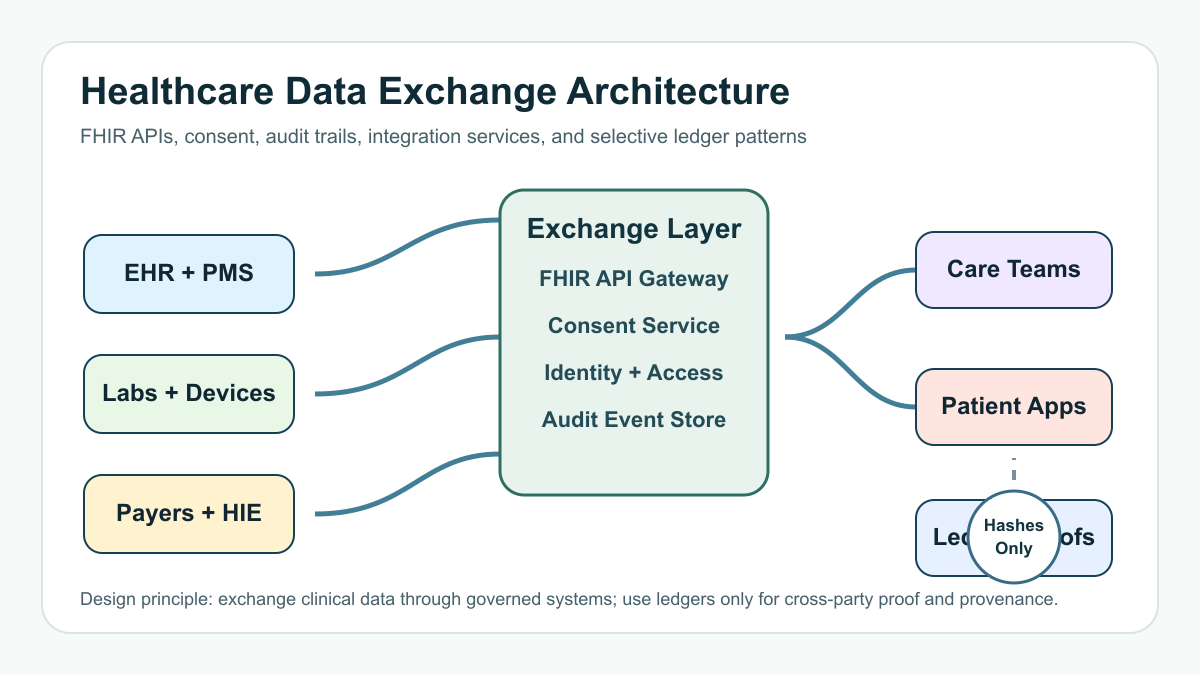

Healthcare data exchange software development is the work of connecting clinical, operational, payer, and patient systems so data can move with the right consent, security, auditability, and context. For most teams, the winning architecture is not "put healthcare on blockchain." It is a governed exchange layer: FHIR APIs where they fit, integration adapters where legacy systems still matter, identity and consent controls, a durable audit trail, and selective ledger patterns only when multiple organizations need shared proof.
The practical question is this: which data should move, who is allowed to request it, what standard represents it, how is consent recorded, and what evidence proves the exchange happened correctly? That is where healthcare data exchange software becomes a business system, not just an API project.
Quick Answer: What Should Healthcare Data Exchange Software Include?
A strong healthcare data exchange platform usually includes a FHIR API gateway, patient and provider identity controls, consent and authorization workflows, interface adapters for EHRs and legacy HL7 feeds, audit logging, monitoring, data normalization, error handling, and operational dashboards. Blockchain is useful only for narrow trust-boundary problems such as consent proof, credential provenance, supply-chain events, or cross-organization audit evidence. Protected health information should normally stay in governed clinical systems, not on-chain.
If you are choosing a partner for this kind of work, evaluate their healthcare security, integration, support, and AI governance practices the same way you would evaluate a healthcare software development company: by proof of process, not generic technology claims.
Why Healthcare Data Exchange Projects Fail
Data exchange projects fail when teams treat interoperability as a single connector. Healthcare workflows are messier. One care pathway may involve an EHR, laboratory system, imaging system, billing platform, claims processor, device feed, care-management tool, and patient app. Each system has its own identifiers, permissions, timing, vocabulary, and data quality problems.
The failure modes are predictable: incomplete patient matching, unclear consent, brittle point-to-point integrations, no replay path for failed events, missing audit context, and dashboards that show uptime but not whether the exchanged data was clinically usable. A data exchange roadmap should begin with workflow evidence: which users need which information, under what authorization, at what moment, and with what downstream decision attached.
Core Architecture for Secure Healthcare Data Exchange
The core architecture has five layers. First, the source systems layer connects EHRs, practice management systems, lab platforms, payer portals, device platforms, and data warehouses. Second, the interoperability layer translates FHIR, HL7, files, webhooks, proprietary APIs, and manual exception queues into a controlled exchange model. Third, the trust layer handles identity, authorization, patient consent, organization policies, and role-based access. Fourth, the evidence layer records audit events, signatures, request purpose, data lineage, and operational alerts. Fifth, the experience layer gives clinicians, operations teams, payers, and patients the screens or APIs they actually use.

Teams planning a broader custom platform should connect this architecture to delivery scope early. NextPage's custom software development work often starts by mapping operating workflows and integration risk before estimating the screens or sprint count.
Where FHIR APIs Fit
FHIR is a healthcare data exchange standard from HL7 that represents clinical concepts as resources and supports modern RESTful API patterns. It is especially useful when a product needs to read, write, or coordinate structured health data in ways that certified health IT, patient apps, analytics systems, and care applications can understand.
FHIR is not a full governance program by itself. A FHIR endpoint still needs authentication, authorization, consent checks, rate limiting, terminology mapping, test data, monitoring, and clear rules for what happens when the target system rejects or partially accepts a request. In production, the hard work is often around identity, workflow semantics, and operational exception handling.
Use FHIR when the exchange maps cleanly to supported resources, when API-based access is required by the ecosystem, or when future interoperability matters. Use HL7 v2, batch files, direct database extracts, event streaming, or vendor-specific APIs when the operational reality requires them. The best exchange systems often support more than one pattern behind a clean internal contract.
Consent and Access Control Are Product Features
Consent is not just a checkbox. It is a product feature with states, scopes, revocation, delegation, expiration, emergency access, and evidence. A patient may approve one provider, one data class, one purpose, or one time period. A payer or health information network may require purpose-of-use declarations. A care team may need break-glass access with additional review.
Build consent as a service that other modules can call before data is disclosed. Store consent decisions, policy version, requester identity, purpose, timestamp, data scope, and revocation state. Then make the user experience clear enough that patients and staff understand what is being shared. If the system has mobile or patient-facing workflows, review related cost and compliance drivers in healthcare app development cost planning before locking scope.
When Blockchain Helps and When It Does Not
Blockchain can help when independent organizations need a tamper-evident shared record and no single party should privately control the proof. Useful healthcare patterns include consent receipts, provider credential attestations, drug supply-chain handoffs, clinical trial provenance, claims event reconciliation, and audit evidence across multiple organizations.
Blockchain is usually the wrong place for raw medical records. On-chain data is hard to delete, expensive to correct, and risky when privacy rules, patient expectations, and data-retention policies change. A safer pattern is to keep protected health information in governed systems and write only hashes, signed references, consent states, or event proofs to a ledger. That lets teams prove integrity without turning the ledger into a clinical database.
Do not use blockchain when one organization owns the workflow, when a conventional database can enforce the audit model, when participants cannot agree on governance, when data correction is frequent, or when the business outcome does not improve because of shared proof. In those cases, spend the budget on APIs, security, monitoring, support tooling, and data quality.
Security and Compliance Planning
Healthcare software that handles electronic protected health information needs administrative, physical, and technical safeguards appropriate to the workflow. The exact implementation depends on the covered-entity or business-associate role, geography, product type, and data class. Treat HIPAA, information blocking, interoperability requirements, device cybersecurity, and payer or network obligations as architecture inputs, not late legal review.
At minimum, scope encryption, access control, MFA, audit controls, backup and recovery, vulnerability management, vendor risk, incident response, logging retention, data minimization, and support procedures. Connected-device or remote monitoring products may also need medical-device cybersecurity planning. Cloud-hosted exchange systems should include workload mapping, network isolation, secrets management, observability, and backup evidence. If infrastructure is a major part of the program, use cloud migration services planning to reduce security and dependency surprises.
Implementation Roadmap
Start with discovery. Map the care or claims workflow, all source systems, all data classes, all actors, and every point where data changes hands. Define the minimum exchange that would improve a measurable outcome: fewer duplicate intake forms, faster referral review, cleaner claims evidence, better discharge follow-up, or safer patient access.
Next, choose the exchange pattern. Decide where FHIR is required, where legacy adapters are unavoidable, where event streaming helps, and where a simple operational dashboard is enough. Build a canonical internal data model only for the concepts your product truly needs. Over-modeling healthcare data is a common way to burn budget without improving care or operations.
Then build the trust layer. Implement identity, organization onboarding, roles, consent, access review, audit logs, and error handling before expanding integrations. Finally, release in phases: one workflow, one set of source systems, one measurable operating outcome, then additional data classes and organizations. A custom software cost estimator can help frame early budget bands, but integration complexity should still be validated through technical discovery.
Cost Drivers for Healthcare Data Exchange Software
The main cost drivers are not the number of screens. They are the number of systems, data standards, user roles, consent states, exception paths, data quality problems, compliance obligations, and operational support requirements. A narrow referral-exchange MVP can be modest compared with a multi-organization platform that handles payer data, patient authorization, EHR writeback, device feeds, analytics, and ledger proofs.
Budget separately for discovery, integration testing, sandbox access, vendor coordination, security review, audit reporting, support operations, and ongoing standards changes. For a broader view of feature and risk estimating, compare the scope against custom software development cost drivers before committing to a fixed roadmap.
Buyer Checklist Before You Build
- Which workflow outcome will the exchange improve first?
- Which systems are authoritative for each data class?
- Which FHIR resources, HL7 feeds, files, or proprietary APIs are actually available?
- Who can request data, for what purpose, and under which consent state?
- How will the system prove access, disclosure, change history, and operational exceptions?
- What data must never leave the system of record?
- Which participants need shared proof that one organization cannot alter alone?
- What support team handles failed messages, duplicate patients, data mismatches, and revoked consent?
How NextPage Scopes This Work
NextPage scopes healthcare data exchange software by separating the workflow, data, trust, and integration problems. That keeps the roadmap practical: first define the operating outcome, then design the exchange layer, then choose whether FHIR APIs, legacy adapters, event logs, or ledger proofs belong in the first release.
If your team is modernizing healthcare data sharing, the useful first step is not a blockchain prototype. It is a secure integration roadmap that shows the source systems, consent model, audit evidence, implementation phases, and cost drivers clearly enough for business and technical stakeholders to approve.